Australian Coding Standards: What Every Coder Needs to Know
Post Author:
TalentMed
 explained")
Classifications Explained
Australian Coding Standards: What Every Coder Needs to Know
The Australian Coding Standards (ACS) are the rulebook that governs how Australian clinical coders apply ICD-10-AM and ACHI. They are the third classification book every coder uses, sitting above the diagnosis and procedure books and deciding which code is the principal diagnosis, when an additional diagnosis is clinically significant, and how codes are sequenced for an episode of care. Published by IHACPA and currently in the Thirteenth Edition 2025, the ACS is the single most consulted reference on a working coder’s desk.
This guide explains what the ACS are, how they are structured, how the rules are applied to a real episode, how the ACS relates to National Coding Advice (NCA), and how coders use the standards day to day. It’s written for career changers, new HLT50321 students, and anyone who wants a clear introduction to Australia’s clinical coding rulebook.

What are the Australian Coding Standards?
The Australian Coding Standards (ACS) are the nationally agreed rules that tell Australian clinical coders how to select, sequence and apply ICD-10-AM diagnosis codes and ACHI procedure codes. Where ICD-10-AM answers “what was wrong?” and ACHI answers “what was done?”, the ACS answers “how should these codes be assigned, in what order, and under what circumstances?”
Every Australian hospital episode is coded against the same ACS, which is what makes the national dataset comparable. Two coders in two different states, reading the same discharge summary, should arrive at the same code set because they are both applying the same standards. Without the ACS, ICD-10-AM and ACHI would produce inconsistent output. With the ACS, they produce a comparable, auditable record that feeds hospital funding (AR-DRG assignment), national health statistics, research, and quality reporting.
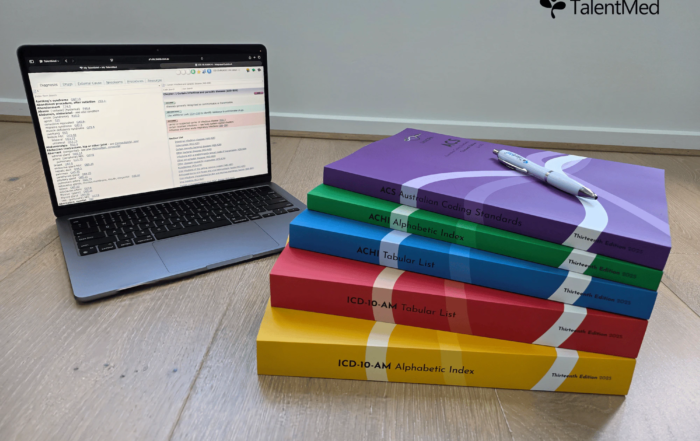
The ACS is a book in its own right, one of the five classification volumes Australian coders use. It sits alongside the ICD-10-AM Alphabetic Index (yellow), the ICD-10-AM Tabular List (red), the ACHI Alphabetic Index (green) and the ACHI Tabular List (blue). Australian coders recognise the ACS by its purple spine.
Who publishes the ACS and why they exist
The ACS is published and maintained by the Independent Health and Aged Care Pricing Authority (IHACPA), the Australian Government agency responsible for national health pricing and classifications. IHACPA was formed in July 2022 when aged-care pricing was added to the remit of the former Independent Hospital Pricing Authority (IHPA). Between 2013 and the transfer to IHPA, the Australian classifications were maintained by the Australian Consortium for Classification Development (ACCD). IHACPA continues the structured edition cycle established under that lineage.
The ACS exists to standardise coding practice across Australia. Before nationally agreed standards, coders in different hospitals made defensible but inconsistent decisions about principal diagnosis, additional diagnoses, and sequencing. That inconsistency undermined the fairness of activity-based funding and the usefulness of the national dataset. The ACS resolves those ambiguities by giving coders a single, auditable rule to apply.
Each new edition of the ACS is developed through public consultation with coders, clinicians, state and territory health departments, and researchers, then released on a scheduled date alongside the matching editions of ICD-10-AM and ACHI. The three books are always used together and are always on the same edition.
How the ACS is structured
The ACS is organised into three parts: General Standards for Diseases (the ICD-10-AM rules), Specialty Standards for Diseases (the body-system chapters that mirror ICD-10-AM), and General Standards for Procedures (the ACHI rules). The Thirteenth Edition 2025 contains 117 individual standards.
Each standard has a standard number (for example 0001, 0002, 0016), a title, and the normative text that coders apply. Coders reference standards by number and title. In a handover, a lead coder might say “I’ve sequenced this as ACS 0001 with the diabetes as principal and the nephropathy as 0002 additional” and every other coder in the room knows exactly what was done and why.
Worked example: applying ACS 0001 to a real episode
The single most important standard is ACS 0001 Principal diagnosis. It defines the principal diagnosis as the diagnosis established after study to be chiefly responsible for occasioning an episode of admitted patient care. Getting ACS 0001 right sets the entire episode up for correct AR-DRG assignment, which is the downstream driver of activity-based funding.
Let’s walk through how a coder applies ACS 0001 to a real episode.
Documentation reads: “Patient admitted via the emergency department with chest pain. Investigations confirmed non-ST-elevation myocardial infarction (NSTEMI). Background of type 2 diabetes mellitus and essential hypertension. During admission, insulin was commenced for stress hyperglycaemia and intravenous glyceryl trinitrate was added on day 1 for elevated blood pressure. Treated with dual antiplatelet therapy and discharged day 4.”
Here is how the coder reasons through the episode:
- 1Identify every documented condition. NSTEMI, type 2 diabetes, essential hypertension. These are the candidates for diagnosis coding.
- 2Apply ACS 0001 to select the principal diagnosis. The condition chiefly responsible for the admission, established after study, is the NSTEMI. The diabetes and hypertension were stable on admission and did not cause this episode. The principal diagnosis is the NSTEMI.
- 3Apply ACS 0002 to test the additional diagnoses. For each secondary condition, check whether it meets one of the three clinical significance criteria: commencement, alteration or adjustment of therapeutic treatment; diagnostic interventions; or increased clinical care. Here, the diabetes qualifies because insulin was commenced for stress hyperglycaemia (alteration of therapeutic treatment), and the hypertension qualifies because intravenous glyceryl trinitrate was added on day 1 (alteration of therapeutic treatment). If both conditions had simply continued on their usual home therapy without change, neither would meet ACS 0002 and neither would be coded.
- 4Look up the codes in the yellow index and verify in the red tabular. The coder navigates to the lead terms and confirms candidate codes in the tabular, reading every relevant chapter, block and category note.
- 5Sequence the final code set. The NSTEMI code is sequenced first as principal diagnosis, followed by the diabetes and hypertension codes as additional diagnoses. Any relevant ACHI procedure codes for interventions performed are added in line with the ACHI standards.
- 6Check ACS 0050 for unacceptable principal diagnoses. Confirm the chosen principal diagnosis code is not on the list of codes that must not be used as principal. An NSTEMI code is an acceptable principal diagnosis, so the episode stands.
That workflow, repeated hundreds of times a week, is the day-to-day job of a clinical coder. The ACS is what turns a thoughtful clinical judgement into a reproducible coded record.
ACS 0002: when is an additional diagnosis clinically significant?
ACS 0002 Additional diagnoses is the second-most applied standard after ACS 0001. It defines when a secondary condition documented in the record should be coded and when it should be left uncoded.
The ACS 0002 test has three clinical significance criteria. A condition is coded as an additional diagnosis when, during the episode, it required any one of: (1) commencement, alteration or adjustment of therapeutic treatment; (2) diagnostic interventions; or (3) increased clinical care. If a documented condition meets none of these, it is not coded. The standard explicitly excludes pre-existing conditions where ongoing medication is simply continued without change: a well-controlled chronic illness that required no new intervention during the admission does not qualify.
ACS 0002 is where over-coding happens. A discharge summary may list ten chronic conditions in the patient’s history, but only a subset meet the clinical significance test for this episode. Applying ACS 0002 rigorously is one of the biggest markers of a careful coder. It is also where auditors focus, because over-coding can inflate complexity and misstate the true resource use of the episode.
ACS and National Coding Advice (NCA): what’s the difference?
The ACS is the published rulebook. National Coding Advice (NCA) is the supplementary guidance IHACPA issues between editions to clarify how a standard should be applied in specific scenarios. The two are separate, and coders use both.
When a real-world coding situation isn’t fully resolved by the standards as written (for example, a new procedure that doesn’t clearly map to an existing ACHI code, or an ambiguous documentation pattern that’s become common), IHACPA publishes an NCA to interpret the existing standards for that situation. NCAs do not overwrite the ACS. They clarify how it applies.
In practical terms:
In a working hospital coding unit, senior coders maintain a current NCA library alongside the ACS book and check both when a tricky episode comes through. The NCA library is a living document that changes between editions.
How coders reference the ACS day to day
Most Australian coders access the ACS through their digital coding software, which integrates the full text of the standards with the ICD-10-AM and ACHI books. A search for a standard number jumps straight to the relevant rule.
Typical daily patterns look like this:
The discipline that separates competent coders from experts is not memorising every standard. It is knowing which standards apply to the case in front of you, and consulting them rather than relying on memory. The ACS is always within arm’s reach for a reason.
The ACS and hospital funding
The ACS is what links a coded episode to hospital funding. Correct ACS application produces a correct AR-DRG assignment; incorrect application produces a wrong AR-DRG and, usually, wrong funding.
AR-DRG (Australian Refined Diagnosis Related Groups) is the national classification that groups episodes of care into clinically and resource-homogeneous categories. The AR-DRG assigned to an episode is driven by the principal diagnosis, the additional diagnoses, the procedures, the patient’s age and discharge status, and the length of stay. All of those inputs come from the coded record, which is built on the ACS. Activity-based funding then applies National Weighted Activity Unit (NWAU) price weights to each AR-DRG to determine the funding the hospital receives.
That is why senior coders and auditors pay so much attention to ACS 0001 and ACS 0002. A principal diagnosis misassignment can shift the episode to a different AR-DRG, which changes the funding the hospital receives. Under-coded additional diagnoses can miss complication and comorbidity that should have contributed to the AR-DRG split. The ACS is not an academic document; it is the operating manual for how Australian public hospitals are funded.
Thirteenth Edition 2025: what’s current
The current edition of the Australian Coding Standards in Australia is the Thirteenth Edition 2025, published by IHACPA and used in lockstep with the Thirteenth Edition 2025 of ICD-10-AM and ACHI.
Edition-to-edition changes typically include revised wording of existing standards to clarify application, new standards that address emerging clinical scenarios, and the incorporation of National Coding Advice that has been issued since the previous edition. When a new edition is released, hospitals update their coding software, train their coders on the changes, and apply the new standards from the implementation date. It’s important to check which edition your employer has implemented and to make sure your reference materials match.
For the authoritative change log between editions, refer to IHACPA’s release notes. The practical point for new coders is simple: you learn and apply the current edition, and you stay alert to NCA updates that appear between editions.
Learning the ACS through HLT50321
Australian coders learn the ACS through the HLT50321 Diploma of Clinical Coding, a 12-month, 100% online qualification designed around real Australian coding scenarios using integrated digital coding software.
The Diploma introduces the ACS alongside ICD-10-AM and ACHI, because the three books are inseparable in practice. Students learn to apply ACS 0001 and ACS 0002 to an episode, to read a specialty standard, to sequence codes correctly, and to decide when to query a clinician for clarification. Because the digital coding software is embedded in the course, you train on the same kind of tools you’ll use on the job, with the full text of the standards at your fingertips.
If you’re considering starting with a lighter introduction, BSBMED301 Interpret and apply medical terminology appropriately is our short-course unit that teaches the medical language you’ll need before or during the Diploma. It is a useful entry point, though it does not qualify you to apply the ACS in a hospital on its own.
Related reading
Start here
Frequently asked questions
Want to find out more?
Speak to a TalentMed course adviser about HLT50321.
12 months, 100% online, flexible payment plans, daily intakes year-round.